Home care is still sold locally. That is not a defect. It is the nature of the trade.
A family does not buy care as it buys accounting software. It buys trust. It asks a neighbour. It calls a retirement-home manager. It listens to a discharge planner. It reads reviews late at night after a parent has fallen, wandered, missed medication or become unsafe alone.
That is why the old home-care growth playbook still works: referral visits, community relationships, local business development, church groups, senior centres, retirement residences and professional referrers. In agency-owner forums, the practical advice is often just as old-fashioned: leave good rack cards in the right local offices, stay visible in the community and build personal referral relationships. The agencies that seem to make this work best do not choose between offline and online. They connect both.
Many Canadian home-care agencies copied the American local-sales model only halfway. They copied the walking, networking and relationship-building. They did not build the digital machinery behind it.
So the owner works harder: more visits, more lunches, more follow-up calls, more driving, more in-home assessments, more manual notes and more promises to “send something tomorrow”.
Meanwhile, the buyer has moved online.
Families search for “home care near me”, “in-home care services”, “dementia care at home”, “companion care for elderly” and “how to find a caregiver you can trust”. The words are plain because the pains are plain: care, trust, speed and control.
The agency that wins the next decade will not abandon local selling. It will connect local trust to a digital front door.
Digital intake, in plain terms, means using the website, forms, phone tracking, CRM, online booking, video assessments, care-plan documentation and follow-up workflows to move a family from first inquiry to first shift with less delay and less manual work. It does not replace local trust. It makes local trust easier to convert, measure and scale.
What home-care agency owners should take from this
Home-care agencies should stop treating digital as a synonym for advertising. The larger prize is digital intake: faster response, better inquiry tracking, online assessment booking, video assessments, AI-assisted care-plan drafting and first-shift verification.
Referrals still matter. A 2023 benchmarking report from Activated Insights found that past and current customer referrals generated more than one-third of revenue across home care, home health and hospice providers. The same report found that providers tracking every inquiry had median revenue more than US$1.2m higher than those that did not, or about C$1.6m.
Video assessments can reduce travel, speed up scheduling, include remote family members and create better documentation when recorded with consent, transcribed and reviewed by a human.
Canadian families are already online
The idea that seniors and family caregivers are mostly offline is outdated. Statistics Canada reported that 95% of Canadians aged 15 and older used the internet in 2022. Among Canadians aged 75 and older, internet use rose to 72%.
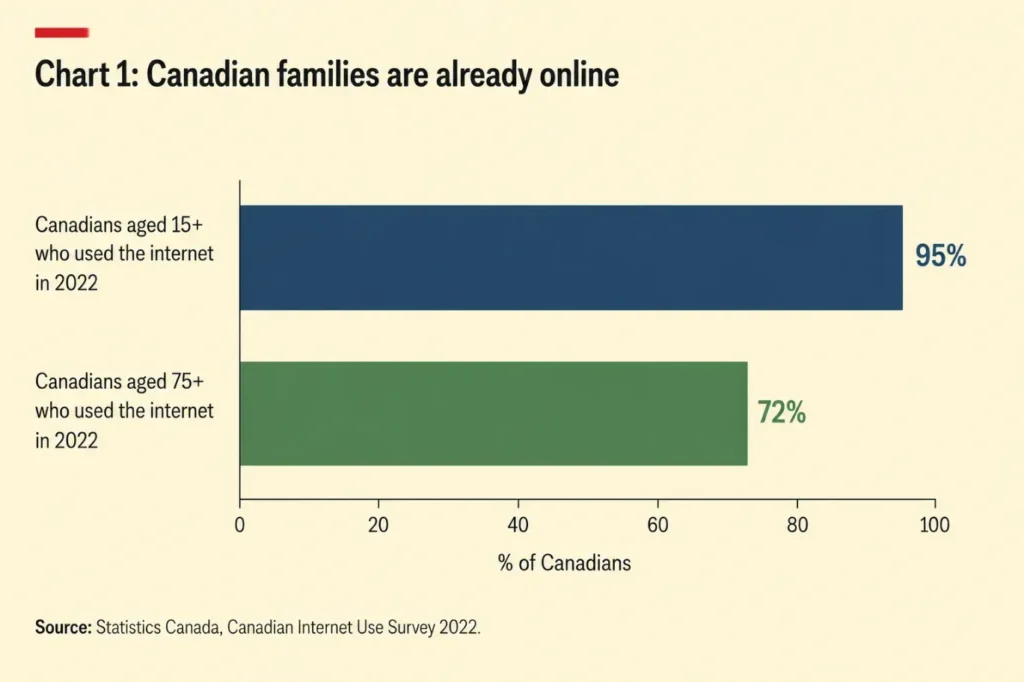
Most Canadian families — including many seniors — are already online, supporting the case for digital caregiving tools, virtual intake, and remote family coordination. Source: Statistics Canada, Canadian Internet Use Survey 2022.
This matters because adult children and many seniors now search, compare, read reviews and book services online before they speak to an agency.
Digital intake is the operating layer between inquiry and admission
Most agencies treat digital as advertising. That is too narrow.
Digital is the operating layer between interest and admission. It captures the inquiry, triggers the call-back, books the assessment, documents the conversation, drafts the care plan, prompts the follow-up and shows which channels produced clients.
Much of the industry advice is useful but shallow. Improve local SEO. Collect Google reviews. Run paid search. Use a home care CRM. Post on social media. Try AI-assisted marketing.
Fine.
But mid-sized Canadian agencies do not need another list of tactics. They need an answer to a harder question: can the agency turn local trust into a measurable intake system without making the owner the permanent salesperson, assessor and follow-up clerk?
Operator discussions point in the same direction. Home-care marketers talk about pairing rack cards and local referral work with a website that ranks in Google, using Facebook not only for client awareness but also for caregiver recruitment, and targeting adult children rather than speaking only to seniors. Treat that as field wisdom rather than formal benchmark data, but it matches the logic of the market: families buy trust locally, then validate it online.
That is where growth usually breaks.
Digital marketing will not fix a leaky intake process
Digital customer acquisition is not cheap. Paid search, lead sites and SEO can all work, but only when the agency has the operating discipline to convert the attention it has bought.
Too often the waste is not in the channel but in the handoff: the unanswered call, the slow reply, the form that lands in an inbox nobody watches, the assessment booked too late, or the coordinator who has to reconstruct a family’s story from scattered notes.
The most economical lead is not necessarily the cheapest one to buy. It is the one the agency is ready to handle.
Industry benchmarking makes the point: reputation, referrals and inquiry tracking remain central to growth. The firms that track every inquiry know what is working. The firms that do not are guessing.
Home-care keywords are getting more crowded
There is another reason paid search deserves caution. Home care does not sit in a quiet advertising category. A family searching for “home care near me”, “PSW care at home”, “dementia care at home” or “in-home care services” may see ads and organic results from private-pay agencies, franchises, lead aggregators, staffing firms, retirement-home brands, health-care providers and large publicly funded or publicly connected organizations.
That matters because Google Ads is an auction. Google says actual cost per click is influenced by competitors and is often tied to the ad rank of the competitor below you. In plain English: the more serious bidders there are for the same intent, the less forgiving the economics become.
In Ontario, home care is not made up only of small private agencies. Ontario Health atHome coordinates local home and community care, long-term-care placement and helps find community services, subcontracting to large, monopoly-like agencies through a prequalification process.
This does not prove that every large publicly funded provider is bidding on the same paid-search keywords as a private agency. Public data does not show that. But it does explain why the search environment feels crowded. To the family, the category is one blurred page of options: public navigation, private care, staffing, senior living, agencies, marketplaces and advice sites. To Google, many of those options can compete for similar search intent.
The practical conclusion is not to avoid Google Ads. It is to avoid using paid search to compensate for weak intake. Bid only where the intent is clear, the landing page is specific, the phone is answered, the assessment can be booked quickly and every inquiry is tracked.
Otherwise a mid-sized agency is not buying growth. It is renting expensive confusion.
Speed comes before ad spend in home-care customer acquisition
Most home-care inquiries are urgent. A daughter calls because something changed. A parent came home from hospital. A spouse is exhausted. A family is arguing about whether care is needed. The caller is not looking for a long education campaign. She wants to know whether the agency can help, whether it can be trusted and how soon the conversation can start.
That means every agency needs a basic digital intake system before it increases marketing spend. At minimum, that means a clear page for each main service and location, a current Google Business Profile, short forms for “home care near me” and “in-home care services” traffic, call and source tracking, a same-day call-back rule, online assessment booking, automated follow-up and a simple CRM pipeline from inquiry to assessment to admission.
This is not glamorous. It is where money leaks.
Your home-care website should behave like an intake desk
Many agency websites still read like printed brochures. They list services, use stock photos and say the agency is compassionate, reliable and professional. So does everyone else.
A better home-care website behaves like a trained intake coordinator. It answers the family’s real questions: whether a parent is safe alone, how quickly care can start, whether dementia care at home is available, what happens after hospital discharge, whether overnight or 24-hour home care is possible, whether a sibling can join the assessment remotely, how caregivers are matched and what happens on the first shift.
This is also how local SEO should work. Thin city pages stuffed with phrases such as “home care near me” or “personal support worker Toronto” will not build trust. Useful local pages that explain care scenarios, service areas, response times, assessment options and next steps will.
Social proof belongs here too. Because home care is a high-trust purchase, testimonials, short family-education articles, caregiver profiles, review snippets and simple videos do more than decorate the page. They reduce the family’s perceived risk. The point is not to produce generic “care tips” for traffic. It is to help an anxious adult child believe the agency understands both the parent’s needs and the family’s decision.
The agency that wins online is not the one with the most keywords. It is the one that makes the family think: these people understand what is happening in our house.
Facebook is useful, but not always in the way owners expect
Google captures active intent. Facebook often creates familiarity before intent becomes urgent. That distinction matters.
Agency owners sometimes judge Facebook too narrowly by immediate client leads. In practice, it can help keep the agency visible with adult children, local families, community partners and potential caregivers. That second audience matters because caregiver recruitment is often the real growth constraint. A consistent Facebook presence can support brand awareness, show the agency’s culture, promote caregiver hiring and make later referral conversations feel warmer.
Online discussions from platforms such as Reddit, among home-care and digital-marketing users reflect this mixed role. Some users describe Facebook and Google ads as ways to reach families actively looking for care; others complain that ads can be slow to generate leads or hard to make profitable, which is why some agencies turn to niche senior-care marketing partners.
The lesson is not that agencies should outsource everything or post more for the sake of it. It is that Facebook, Google, SEO, rack cards and referral visits should be part of one system, not five disconnected experiments.
Video assessments can shorten the path from inquiry to care plan
The in-home assessment has become almost sacred in home care. It feels professional. It feels personal. It reassures the family. It lets the agency see the home.
Sometimes it is necessary. Often it is also costly, slow and awkward.
A coordinator or nurse must schedule the visit, drive to the home, park, complete the assessment, return, write notes, create a care plan and follow up. If the adult child lives in another city, they may not be there. If the visit is rescheduled, the sales cycle stretches.
Virtual care is now familiar enough to support a digital-first assessment model. Statistics Canada found that 78.5% of people who sought or were offered virtual care in 2023 had a virtual appointment. Fewer than one in ten declined one; among those who declined, technology-related concerns were not commonly reported.
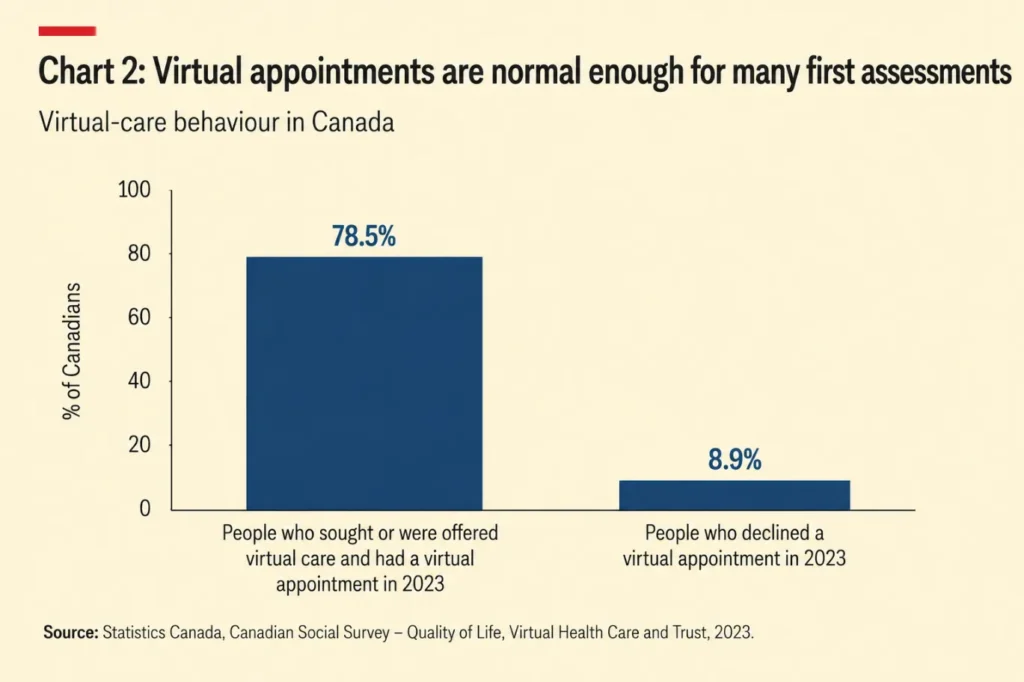
Virtual care has become mainstream in Canada, with most patients accepting virtual appointments when offered. This creates opportunities for home-care agencies to streamline intake and assessments digitally. Source: Statistics Canada, Canadian Social Survey – Quality of Life, Virtual Health Care and Trust, 2023.
In our experience at ConsidraCare, almost every family accepts a video assessment when it is explained properly. I would not publish “99%” as a market statistic unless it has been formally tracked. But the pattern is clear: families are often relieved when they can meet sooner, include siblings or adult children from other cities, and avoid waiting for an in-home slot.
A video assessment is not a lower-quality assessment. Done properly, it is a faster, better-documented first step.
A video assessment should create structured notes, not just another meeting
Done badly, a video assessment is just a meeting. Done well, it becomes an operating workflow.
A structured video assessment can be recorded with consent, transcribed, summarized and turned into a draft care plan. The family can share context. The decision-maker can join remotely. The agency can capture risks, routines, preferences, medications, mobility needs, dementia concerns, meal support, bathing requirements, family expectations and start-date urgency.
A human should then review the output before anything becomes final.
This is where AI is useful. Not as theatre, and not as a chatbot pretending to understand care, but as an administrative assistant that turns a messy conversation into structured notes, visit instructions, care-plan tasks and follow-up actions.
For owners searching for “home care documentation software”, “care notes app”, “caregiver mobile app” or “home care CRM”, this is the point: the value is not the software label. The value is less rework, fewer missed details and faster care-plan creation.
Privacy still matters. Recording, transcription and AI summaries must be consent-based, securely stored and reviewed by the right person. AI should draft. The agency should decide.
The home still needs a safety check, but not always before the first conversation
The strongest objection to video assessments is the home-safety check. Some things are easier to see in person: stairs, rugs, bathrooms, lighting, clutter, mobility hazards, fridge contents, medication location, walker fit and transfer risks.
But this does not mean the first assessment must always happen in person. A practical model is hybrid. The first assessment happens by video, quickly. The care plan is drafted immediately. The first caregiver shift includes a structured home-safety checklist. Any red flags are escalated to the supervisor. The care plan is updated after the first shift.
This works only if the caregiver has the right mobile workflow: checklist, note-taking, supervisor escalation, care-plan updates and clear permissions for any photos or documentation. Without technology, the safety check becomes another loose piece of paper. With the right caregiver mobile app and home care documentation workflow, it becomes proof that the agency did what it said it would do.
The economics of digital assessments are better than most owners think
Consider a simple model. An in-home assessment takes 90 minutes in the home, 45 minutes of round-trip travel, 20 kilometres of driving and 30 minutes of write-up. At a loaded coordinator cost of C$35–C$50 per hour, plus mileage, the agency’s internal cost can easily reach C$111–C$153 before the client has started care.
A video assessment may take 60–75 minutes, eliminate travel and reduce write-up time if the meeting is transcribed and converted into a draft care plan.
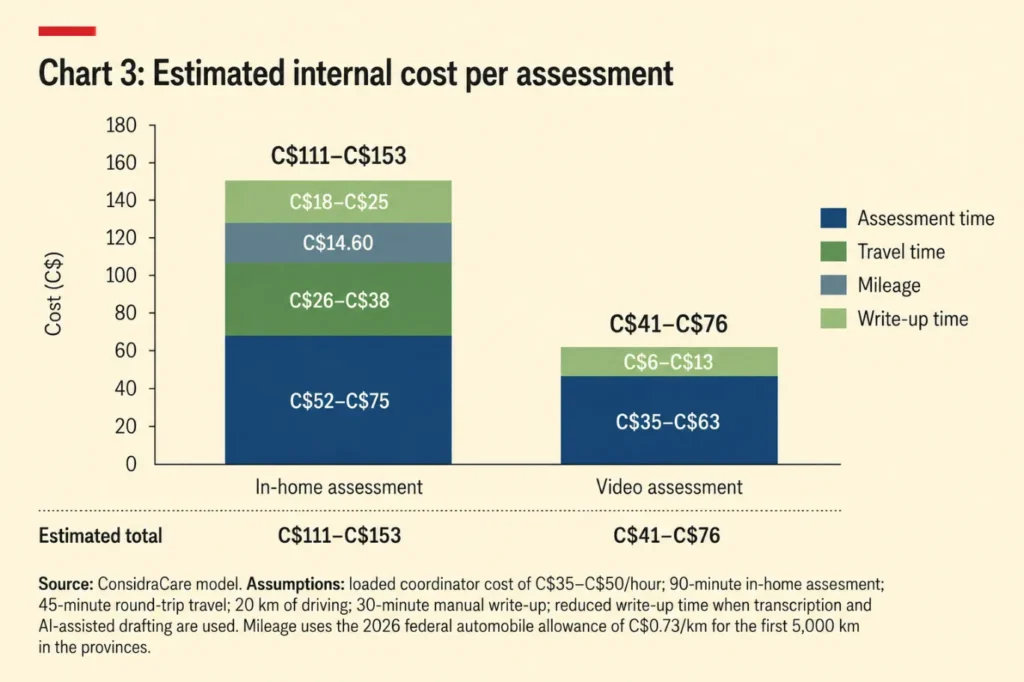
Video assessments can significantly reduce operational costs for home-care agencies by eliminating travel and lowering documentation time through transcription and AI-assisted workflows. Source: ConsidraCare operating model assumptions.
Even if the real saving is lower, the direction is clear. If an agency completes 40 assessments a month and moves half to video, saving C$50 per assessment, it avoids C$1,000 a month in assessment cost. More importantly, it may shorten the time from inquiry to assessment.
Speed matters. Families rarely wait patiently while an agency gets organized. If one provider can assess today and another can assess next week, the first provider has an advantage.
The home-care sales funnel is really an operating system
The intake funnel is simple: an inquiry becomes an assessment, an assessment becomes an admission, an admission becomes a first shift, and a first shift becomes a stable client relationship or a complaint. That is the spine of a serious agency growth system.
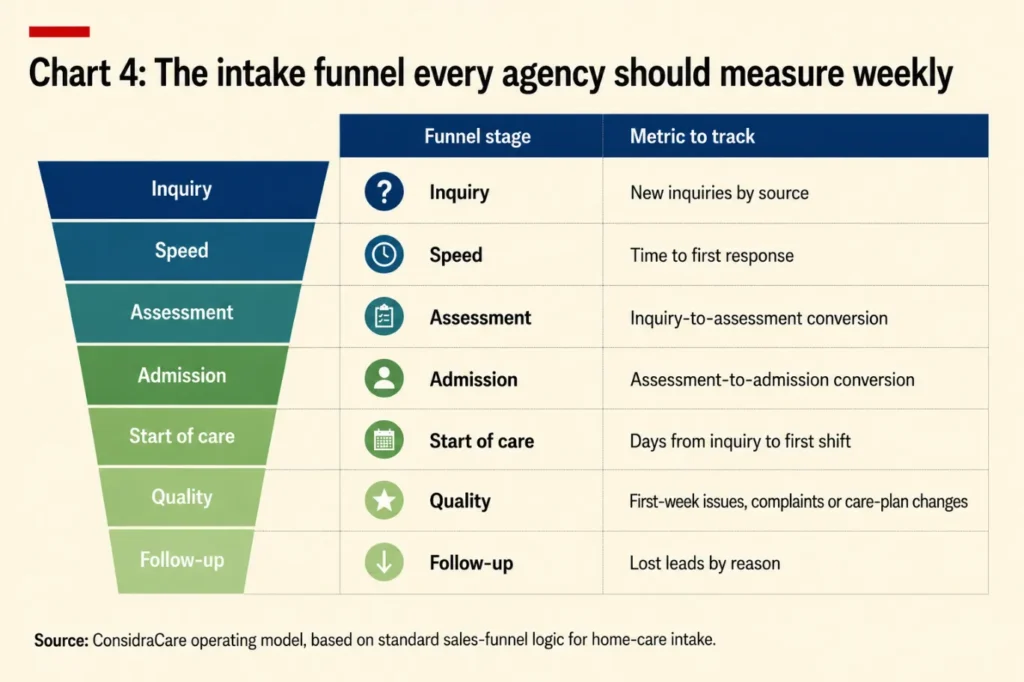
Tracking intake funnel performance weekly helps home-care agencies improve response speed, conversion rates, operational quality, and caregiver scheduling efficiency. Source: ConsidraCare operating model based on standard home-care intake funnel logic.
This is what an owner should review every Monday: not likes, impressions or vague brand awareness, but where qualified inquiries came from, how fast the agency responded, how many booked assessments, how many became clients and where the process broke.
That is home-care agency marketing for grown-ups.
The agency owner should not be the CRM
In many agencies, the owner is the system. The owner remembers the referral source, knows which daughter is anxious, knows which caregiver fits which client, follows up with the warm lead, senses which assessment is likely to close and notices when a family goes quiet.
That can work at ten clients. It does not work at scale.
A mid-sized agency needs the knowledge to live in the operating system, not in the owner’s head. Every inquiry should have a source, stage, owner, next action, assessment status, care-plan status and close reason. Every lost opportunity should teach the agency something.
Searches for “home care CRM”, “home care scheduling software”, “caregiver scheduling app”, “home care billing software” and “home care communication platform” are really symptoms of the same disease: the agency has outgrown memory.
The answer is not just another tool. It is a connected workflow.
What digital intake means for Canadian home-care agencies
Canadian home care has its own reality. It is local, trust-based and fragmented. The public system, private-pay market, retirement-home ecosystem and hospital-discharge pressures differ by province and city. A tactic copied from a large American franchise will not automatically work in Mississauga, Ottawa, Calgary, Halifax or Vancouver.
But the operating truth is the same. The agency that depends only on shoe-leather selling will become tired. The agency that depends only on digital ads will become expensive. The agency that connects the two will become stronger.
Local relationships create trust. Digital systems capture and convert that trust. Video assessments shorten the sales cycle. AI-assisted documentation reduces rework. Mobile first-shift checklists protect quality. Tracking shows the owner what is working.
That is the shift: not from human care to digital care, but from owner-dependent growth to system-supported growth.
Start by measuring inquiries, assessments and admissions
Do not start by buying more ads. Start with four questions: how many inquiries did the agency receive last month, by source; how quickly did it respond; how many became assessments; and how many assessments became clients?
Then ask four more: how many assessments could have been done by video; how much coordinator travel time was spent; how long care-plan creation took; and how many first-week issues could have been prevented with a better digital handoff?
If the answers are unclear, the agency does not have a marketing problem. It has an operating-system problem.
Take the free agency audit or join the ConsidraCare partner pilot
If you own or operate a home-care agency and growth still depends too much on manual follow-up, in-person assessments, disconnected tools or the owner personally holding the process together, start with our free agency operations audit:
Take the free agency audit: https://considracare.com/agency-audit/
ConsidraCare is also looking for a small number of founding partner agencies to co-build a more digital operating model for intake, assessment, care-plan creation, first-shift verification, family communication and management reporting.
Register interest in the partner pilot: https://considracare.com/book-operational-review/
The goal is not to make home care less personal. It is to stop wasting the owner’s time on work that better systems can do.