Home care agencies do not usually break because nobody wants care. They break because the agency cannot reliably turn demand into delivered shifts.
The owner wins a referral. The family books an assessment. The recruiter finds a caregiver. The care plan looks workable. Then the schedule has to make all of it real: the right caregiver, the right client, the right time, the right skills, the right travel time, the right notes, the right family expectations and the right supervisor backup.
That is where many growing agencies start to crack.
The scheduler is expected to absorb every upstream weakness. Intake was rushed. Availability is stale. The client prefers mornings. The caregiver wants weekdays. Travel time has been underestimated. The care plan is vague. A family changes the visit time. A caregiver calls in sick. Another stops replying. The phone rings, the calendar turns red and the owner wonders why growth feels so much like emergency dispatch.
Scheduling is not clerical work. It is the operating centre of home care.
For Canadian agencies, this matters because geography is unforgiving. A schedule that looks reasonable on a spreadsheet can become expensive in the GTA, the Lower Mainland, Ottawa, Calgary or a rural service area where ten kilometres can mean 25 minutes at the wrong time of day. The question is not simply how to fill home care shifts. It is how to build a system that keeps care reliable without burning out schedulers, caregivers and margins.
What home-care agency owners should take from this
Home-care scheduling problems are rarely just scheduling problems. They are the visible result of weak intake, thin care plans, incomplete caregiver profiles, poor availability data, bad routing, weak bench strength, missing shift alerts and unclear family communication.
The better agency does not treat scheduling as a heroic daily rescue act. It treats scheduling as a data problem, a matching problem and a service-execution problem. Human judgment still matters, but it should not have to compensate for missing information every hour.
A scheduling calendar software is not the right tool. The stronger idea is an operating platform: intake, caregiver onboarding, scheduling, care plans, mobile shift execution, family communication, reporting, SOPs, templates, AI support and proof-of-service workflows in one operating model, such as offered by ConsidraCare.
Scheduling is where the agency’s promises become real
The website can promise reliability. The recruiter can promise good caregivers. The owner can promise peace of mind. But the schedule decides whether care actually happens.
Families judge reliability at the door. Did the caregiver arrive? Did they know the care plan? Did they stay the right amount of time? Did someone call when plans changed? Did the agency notice the problem before the family did?
That is why scheduling affects more than operations. It affects reputation, retention and revenue. A missed or badly handled shift can turn a new client into a complaint. A poor caregiver match can turn a good hire into a resignation. A route with too much travel can turn a profitable day into a thin-margin day.
Research on home-health routing and scheduling makes the same point in operational terms: routing, scheduling and workload balance affect cost, care delivery and service quality.
Missed visits make scheduling a quality and risk problem
A weak schedule does not merely inconvenience the office. It can create a care-quality problem.
In home care, reliability is part of the service. A visit that starts late, changes without warning or does not happen at all affects the client’s routine, the family’s trust and the caregiver’s workload. For higher-need clients, the consequences can be more serious: missed meals, delayed personal care, medication concerns, fall-risk exposure or an anxious family calling the office because nobody told them what changed.
Ontario’s Retirement Homes Regulatory Authority and system partners published guidance in 2024 to reduce the negative effects of missed home-care visits in retirement homes. The guidance focuses on risk assessment, contingency planning, communication and tracking when visits are missed or disrupted.
Client and caregiver feedback points in the same direction. A Health System Performance Network report on Ontario home and community-care experience found that communication, continuity, timing, safety and service-provider issues showed up repeatedly in client and caregiver feedback.
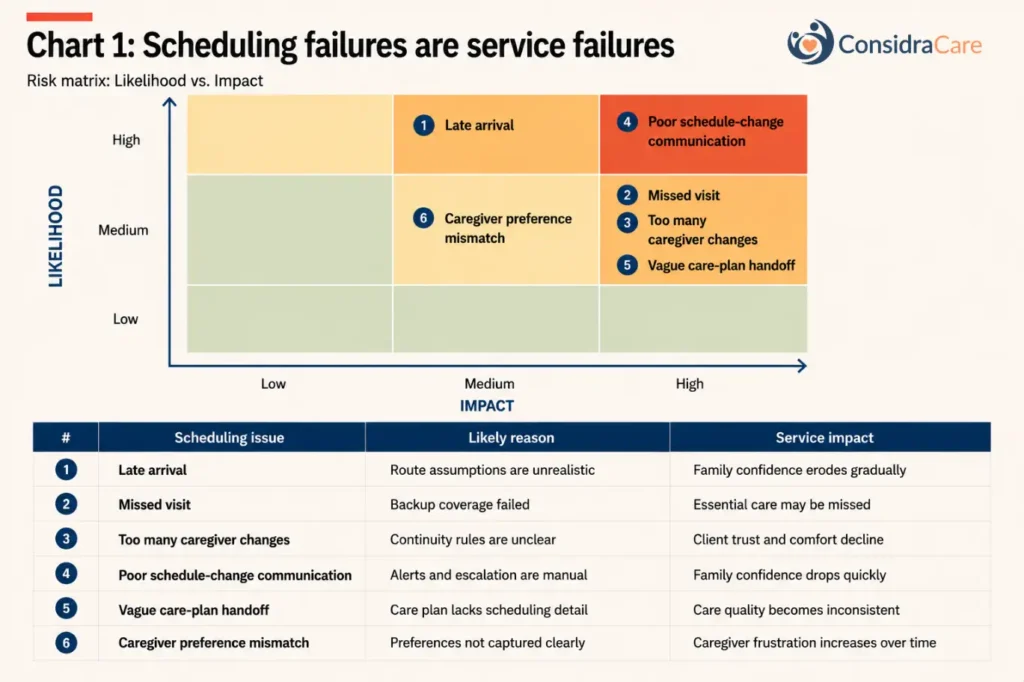
The practical point is uncomfortable but useful. Scheduling should not be measured only by whether the calendar is full. It should be measured by whether care was delivered on time, by the right caregiver, with the right instructions, and whether the agency saw problems before the family had to call.
Most scheduling problems start before the schedule
A scheduler can only work with the inputs the agency gives them. If those inputs are poor, the schedule will be poor.
The first bad input is intake. If the assessment does not capture location, timing constraints, family expectations, care complexity, risk level, language preferences, mobility needs and likely visit duration, the scheduler inherits a guessing game.
The second is caregiver data. Skills, credentials, travel radius, availability, preferred hours, client preferences, dementia experience, lift-transfer comfort, driving status and willingness to do evenings or weekends should not live in someone’s memory.
The third is care-plan quality. A vague care plan makes matching harder. “Companionship and personal care” may be enough for a brochure, but it is not enough for a scheduler deciding whether a caregiver is ready for a client with dementia, fall risk, incontinence, family anxiety and a narrow visit window.
This is why “best-fit matching” cannot be solved by a calendar alone. The match depends on the quality of the data behind the calendar.
Travel time is where margin quietly leaks
Canadian home care is a mobile-service business. That sounds obvious until an agency prices and schedules as if caregivers teleport.
Travel time, idle gaps and short shifts can quietly ruin the day’s economics. Ontario’s employment-standards guidance says time spent travelling during the course of the workday between shifts is considered work time. Caregivers on payroll need to be compensated for at least 3 hours even if the shift is shorter. Agencies should still get payroll and legal advice for their own arrangements, especially where employment status, on-call work, breaks, collective agreements or contractor relationships are involved.
For mileage, the federal 2026 automobile allowance rate for the provinces is C$0.73 per kilometre for the first 5,000 kilometres and C$0.67 after that.
Table 1: How travel and idle time can erase margin
| Scheduling scenario | Visit revenue | Direct caregiver time | Travel / idle cost | Mileage cost | Gross margin before overhead |
|---|---|---|---|---|---|
| Tight local route: two 2-hour visits, 15 minutes between homes, 8 km travel | C$160 | C$88 | C$6 | C$5.84 | C$60.16 |
| Loose route: two 2-hour visits, 45 minutes between homes, 22 km travel | C$160 | C$88 | C$19 | C$16.06 | C$36.94 |
| Broken route: two 2-hour visits, 90-minute gap, 30 km travel | C$160 | C$88 | C$38 | C$21.90 | C$12.10 |
Source: ConsidraCare model. Assumptions: C$40/hour client billing, C$22/hour caregiver wage, travel/idle time costed at C$25/hour, mileage at C$0.73/km. Adjust to local rates, worker classification and payroll rules.
The exact numbers will vary. The pattern will not. A schedule with the wrong geography can look full and still produce weak margin. That is why zone-based scheduling is not a small improvement. It is a margin strategy.
Zone-based scheduling reduces chaos before it reaches the desk
Many owners try to schedule the whole city as one territory. That is understandable when the agency is small. It becomes costly as the agency grows.
A better model is to divide the service area into zones and build caregiver capacity inside each zone. The aim is not to draw beautiful maps. It is to reduce the daily friction of travel, lateness, refusals and last-minute replacements.
Operator discussions often point to a practical rule: keep caregivers within a reasonable radius of their home, previous shift or preferred working area wherever possible. I would not treat claims such as “30% fewer late arrivals” as a benchmark unless an agency has measured it. But the operating logic is sound. Less travel uncertainty means fewer late arrivals, more acceptable shifts, better caregiver satisfaction and lower scheduler stress.
Zone-based scheduling works best when the agency tracks the right data: caregiver home area, travel radius, driving status, public-transit constraints, preferred zones, client locations, visit windows, historical lateness and cancellation patterns. Without that data, the zone map becomes another poster on the wall.
Last-minute shifts are a system problem, not a daily surprise
Some emergencies are unavoidable. People get sick. Families change plans. Caregivers have car trouble. Weather turns ugly.
But if every week depends on a scheduler calling 30 or 40 people in panic, the agency has a system problem. The real issue may be weak bench strength, poor forecasting, stale availability, over-reliance on a few caregivers, part-time workers with competing jobs or a failure to identify fragile shifts before they break.
The better model is a tiered coverage system. Agencies can maintain a small on-call bench for high-risk periods, such as mornings, evenings, weekends, holidays and complex-care blocks. In some cases, an agency may pay a standby amount to one or two caregivers, then use them for wellness calls, documentation cleanup, training refreshers or other useful work if no shift breaks. The details depend on local employment rules and agency economics. The principle is clear: do not make reliability depend on desperate phone calls.
Missed visits should be treated as operational exceptions with a root cause, not as ordinary turbulence.
The cost of a missed shift is larger than the lost revenue
Agency owners often calculate a missed shift too narrowly. They see the lost four hours of revenue. That is only the obvious cost.
A missed shift can create overtime, emergency replacement cost, supervisor time, family complaint handling, caregiver frustration and reputational damage. In the worst case, the client leaves and the agency loses the lifetime value of the account.
Table 2: The real cost of one missed four-hour shift
| Cost item | Conservative estimate | Calculation |
|---|---|---|
| Lost revenue from missed four-hour visit | C$160 | 4 hours × C$40/hour |
| Scheduler and supervisor recovery time | C$40–C$80 | 1–2 hours × C$40/hour |
| Emergency replacement premium or overtime risk | C$25–C$75 | Extra pay, travel or short-notice premium |
| Family complaint follow-up | C$25–C$75 | Admin and manager time |
| Potential revenue at risk if client churns after repeated failures | C$3,200–C$12,800+ | 5–20 weeks × 4 hours/week × C$160/week |
This is the “aha” many owners need. The scheduling desk is not just protecting today’s shift. It is protecting the client relationship.
Best-fit matching should be structured, not random calling
Every experienced scheduler has instincts. They know who is reliable, who can calm anxious families, who handles dementia well, who dislikes long drives and who will accept an evening shift if asked properly.
That judgment is valuable. It should not be trapped inside one person’s head.
Best-fit matching should use structured criteria: skills, credentials, language, geography, availability, client preferences, caregiver preferences, risk level, continuity, travel time, documentation history and past attendance. The scheduler still makes the decision, but the system should narrow the field intelligently.
This matters for caregiver retention. A bad match tells the caregiver that the agency does not understand their limits. It also tells the family that the agency does not understand the client. Repeated bad matches turn into churn on both sides.
The goal is not to automate care judgment away. It is to stop wasting human judgment on preventable searching.
Client consistency and caregiver preference are always in tension
Every agency owner knows the impossible preference map. Families want the same caregiver, at the same time, with no disruption. Caregivers want steady hours, close-to-home work, manageable clients and often weekday daytime shifts. The agency wants margin, reliability and enough flexibility to cover the week.
Those preferences cannot all win all the time. The scheduling desk is where the trade-off becomes visible.
The mistake is to pretend the trade-off does not exist. A better agency sets rules. Some clients need continuity above all else: dementia clients, complex personal care, palliative support or families with high anxiety. Some shifts need flexibility: light companionship, short relief visits or cases where the client accepts a small care team. Some caregivers should be protected from poor matches because losing them would be more costly than moving a shift.
Scheduling policy should make these choices explicit. Otherwise, every decision becomes a negotiation, and every negotiation lands on the scheduler.
Scheduler burnout is a warning light for the whole agency
When a scheduler burns out, owners often treat it as a staffing issue at the desk. Sometimes it is. More often, it is a sign that the operating system is overloaded.
The scheduler is dealing with late arrivals, caregiver call-outs, family complaints, unclear care plans, inconsistent availability, last-minute admissions, route problems, documentation gaps and owner pressure. If the agency has no reliable data, no escalation rules and no clear coverage model, the scheduler becomes the shock absorber for the whole company.
That is not sustainable. A burned-out scheduler creates more errors, slower responses and worse communication. The agency then needs another heroic scheduler, and the cycle repeats.
The solution is not merely to hire a tougher person. It is to reduce the number of decisions that require heroics.
Mobile execution is where the schedule proves itself
A schedule is only a plan until the caregiver arrives and checks in.
Agencies need proof that the visit happened, that the caregiver knew what to do, that notes were captured, that changes were escalated and that the family was informed when needed. This is where mobile caregiver apps, shift notes, alerts, checklists, GPS check-ins where appropriate, visit verification and family communication become part of the scheduling system.
Without real-time visibility, the agency often learns about a problem from the family. By then, the agency is no longer managing service quality. It is managing damage.
The strongest model is scheduling plus execution: a schedule connected to care plans, caregiver profiles, mobile shift documentation, missed-visit alerts, family notifications, incident workflows and management reporting.
That is the difference between a calendar and an operating system.
A better scheduling operating model for home-care agencies
A stronger scheduling model has six parts.
First, intake must capture scheduling reality, not just care needs. Visit windows, parking, access instructions, family expectations, language, pets, mobility risks, preferred routines and likely visit duration all matter.
Second, caregiver profiles must be complete and current. Skills, credentials, availability, geography, transportation, preferences and restrictions should be structured data, not notes scattered across texts and spreadsheets.
Third, the agency should use zone-based scheduling wherever possible. It should know which caregivers can serve which areas, which visits create bad routes and which geographies are unprofitable without minimum visit lengths or adjusted pricing.
Fourth, the agency should create a coverage bench. High-risk periods deserve planned backup, not frantic improvisation.
Fifth, the schedule should feed the mobile workflow. The caregiver should see the care plan, tasks, risks, route notes, documentation requirements and escalation path before the visit starts.
Sixth, management should review scheduling KPIs weekly. The owner should know late arrivals, missed visits, unfilled shifts, travel time, overtime, caregiver refusals, client continuity and scheduler workload.
The weekly scheduling dashboard owners should use
Many agency owners review revenue, new clients and open shifts. Those numbers matter, but they do not show whether scheduled care is actually being delivered as promised.
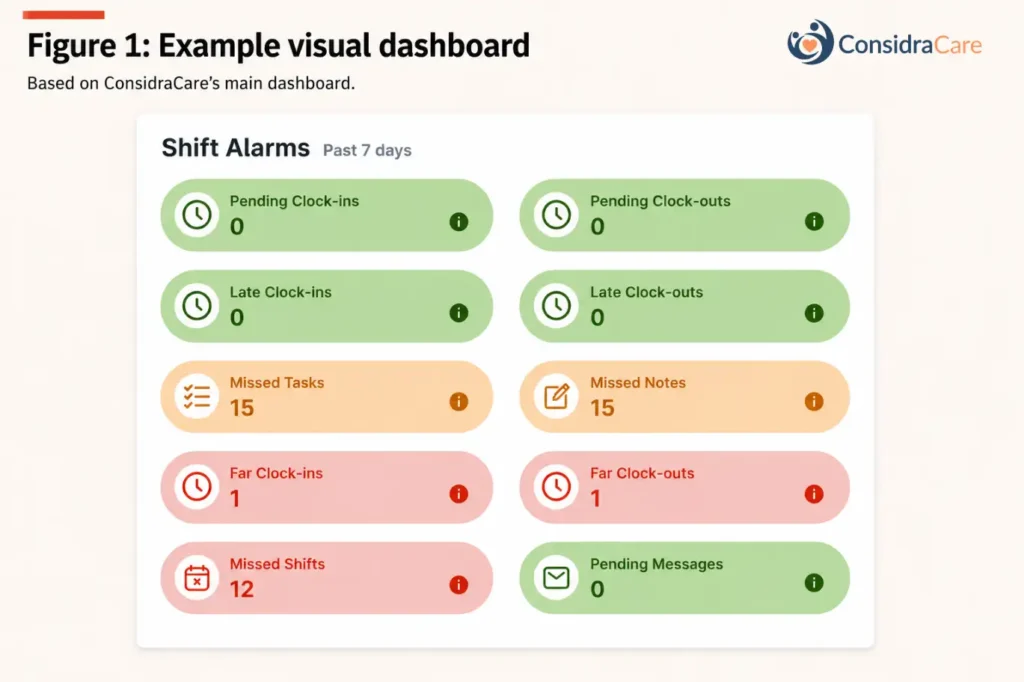
A useful scheduling dashboard should work less like a calendar and more like an early-warning system. It should surface exceptions before they become complaints: visits that may not have started, visits that closed late, missed tasks, missing notes, location mismatches and messages that still need a response.
ConsidraCare’s shift-alarm view follows this logic. It separates routine scheduling from operational risk. Pending clock-ins suggest a visit may be at risk. Late clock-ins reveal punctuality or routing problems. Missed shifts show service failure. Missed tasks and missed notes show whether care was both delivered and documented. Far clock-ins or clock-outs can flag location, routing or compliance issues. Pending messages show communication delays before they become family frustration.
Table 3: The scheduling dashboard every owner should review weekly
| Dashboard signal | What it reveals | Owner question |
|---|---|---|
| Pending clock-ins | Visits may not have started | Which shifts need immediate follow-up? |
| Late clock-ins | Routes or schedules may be unrealistic | Are lateness patterns tied to geography or workload? |
| Pending clock-outs | Visits may not have closed properly | Are caregivers completing shift workflows? |
| Late clock-outs | Visits may be running over or closing late | Are care plans or visit lengths realistic? |
| Missed shifts | Service delivery failed | Was backup coverage triggered fast enough? |
| Missed tasks | Care may be incomplete | Which clients or caregivers need review? |
| Missed notes | Documentation is missing | Are we losing proof of service? |
| Far clock-ins / clock-outs | Location or routing may be wrong | Are addresses, routes or check-ins reliable? |
| Pending messages | Communication is delayed | Which caregivers need a response? |
Source: ConsidraCare operating model, based on shift alarms for clock-ins, clock-outs, missed shifts, missed tasks, missed notes, location exceptions and pending messages.
The purpose is not to punish schedulers or caregivers. It is to identify the weak points in the operating system. Late clock-ins may point to bad routing. Missed notes may point to poor mobile-documentation habits. Missed tasks may point to weak care-plan handoff. Far clock-ins may point to address, training or compliance issues. The owner’s weekly question should be: which exceptions were isolated, and which are becoming patterns?
What scheduling control means for Canadian home-care agencies
Canadian home care is a trust business, but trust still has to be scheduled, routed, documented and delivered.
That is why a growing agency eventually outgrows heroics. One talented scheduler can hold the business together for a while. They know the caregivers, remember family preferences, sense fragile shifts and rescue the day with enough calls and texts. But that model has a ceiling. When client volume grows, geography spreads and caregiver availability becomes more variable, memory stops being a system.
Scheduling control means the agency can see the work clearly enough to manage it. It knows which shifts are fragile before they break. It knows which routes are unrealistic. It knows which clients need continuity and which visits can tolerate flexibility. It knows when care was delivered, when documentation is missing and when the family needs a call.
That is the shift: not from human judgment to automation, but from filling shifts by instinct to managing delivery with evidence.
Start by finding the scheduling leaks
Do not start by buying another standalone calendar. Start by finding where the current schedule leaks.
Look at the last 30 days. Which shifts were hardest to fill? Which areas created the worst routes? Which clients generated the most schedule changes? Which caregivers refused the most shifts, and why? Which visit windows were unrealistic? How much travel time was paid, absorbed or ignored? How many missed visits were caught by the agency before the family complained? How often did the scheduler work after hours?
Then look for patterns rather than anecdotes. A single late arrival may be bad luck. Repeated late arrivals in one zone suggest bad routing. A single missed note may be forgetfulness. Repeated missed notes suggest weak mobile workflow or poor training. One caregiver refusal may be normal. Repeated refusals for the same client may mean poor matching, unclear care-plan expectations or unrealistic visit timing.
If the agency cannot answer these questions, it does not have a scheduling software problem alone. It has an operating-system problem.
To make this practical, we built the ConsidraCare Scheduling Control Toolkit as a companion to this article. It includes six working tools to help agency owners diagnose scheduling leaks, triage shift risks, plan service zones, improve caregiver matching, standardize first-shift handoffs and review weekly scheduling exceptions before families complain. Download the toolkit and use it with your scheduler or operations lead to find where your calendar is really breaking.
ConsidraCare_Home_Care_Scheduling_Control_Toolkit